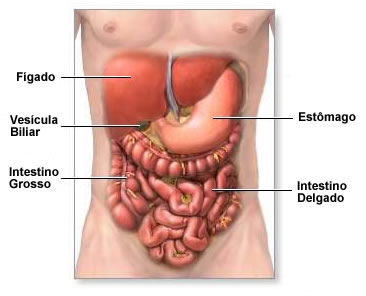
INTESTINO GRUESO
Se extiende desde la válvula ileocecal hasta el ano, mide unos 1.8 metros de longitud con variaciones individuales sin importancia, diámetro variable entre 2 a 3 cm en sigmoides y 6 a 8 en ascendente.
Irrigado básicamente por la mesentérica superior, cólica media, cólica derecha e izquierda (arco de Riolano) que constituyen las arterias terminales o marginales. Las venas igual nombre. El recto por las hemorroidales superior, inferior y media. Fisiológicamente es un gran reservorio, su mucosa es lisa, le llega entre 500 a 700 cc de agua de la cual se absorbe un mínima parte. Tiene haustras destinada a hacer más lento el paso del contenido y así favorece el contacto con la mucosa.
ST ATRIBUIBLES
• DOLOR generalmente localizado en marco colónico, sigma y recto en región suprapúbica. Relacionado o no con la defecación.
• PUJO – TENESMO sensación de evacuación incompleta y ganas de evacuar.
• HEMATOQUEZIA sangre viva
• PROCTORRAGIA heces fecales y sangre
• DIARREA
• CONSTIPACION
METODOS DE DX
Estudio de la materia fecal - tacto rectal
Rectosigmoidoscopia
Colonoscopia convencional - Capsula endoscópica.
Radiologia (colon per – oral o colon por enema doble contraste).
Tac – colonoscopia virtual por tac
Ecografia
Angiografia - centellografia
ENFERMEDAD DIVERTICULAR DEL COLON
Descrita en 1804 por Voigtel, se define como un trastorno estructural caracterizado por la formación de pequeñas hernias de la mucosa a veces sin participación de todas las capas del intestino haciendo protrusión a través de la pared colónica.
Se presenta en etapas avanzadas de la vida, similar incidencia en relación al sexo, 90 a 95 % afecta colon sigmoides.
Se atribuye a debilidad muscular y aumento de la presión intraluminal.
ST: generalmente asintomático, el paciente se puede quejar de dispepsia, náuseas, diarrea, estreñimiento, síntomas urinarios; pero sí los hay cuando se presentan complicaciones (diverticulitis, absceso, perforación o hemorragia).
DX: evaluar los síntomas, fundamentalmente es radiológico de doble contraste pero complementado con colonoscopia para descartar patología asociada, ecografía o mejor aún tomografía con contraste VO y EV.
TTO: dieta rica en fibra, hidratación adecuada.
COMPLICACIONES: DIVERTICULITIS Dieta, reposo intestinal, antibióticos VO o EV según el caso.
- ABSCESO antibióticos EV y dieta cero.
- FÍSTULA indicación de cirugía.
- PERFORACION indicación de cirugía.
- HEMORRAGIA tratamiento médico y cirugía en caso de fracaso con el tratamiento médico instaurado.
TU DE COLON
BENIGNOS o POLIPOS (griego pulpos y en latín octopos). Se clasifican en:
Neoplasicos - Adenoma “ tubular, velloso y mixto”, poliposis familiar o adenomatosis, carcinoide, poliposis linfoide maligna.
No Neoplasicos - Hamartomas (Sme de Peutz Jegherz), poliposis juvenil, Inflamatorios (poliposis linfoidea benigna), misceláneos (lipoma, leimioma, fibroma).
ADENOMA: el más frecuente es el Tubular generalmente pediculado con mucosa similar, tenemos el Velloso o papilar generalmente sésil de superficie frondosa cerebroide, aterciopelado.
CLINICA: silenciosa, hemorragia, mucoquezia, diarrea.
DX: endoscópico, clasificación de Yamada I II III IV.
TTO: resección endoscópica, cirugía. Pueden evolucionar hacia el CA Colorectal. Polipectomia, mucosectomia (CA temprano de colon)
TU MALIGNOS DE COLON
El 98 % son adenocarcinomas, el 2 % otros tumores.
CA COLORECTAL
Más frecuente en países occidentales (Europa Occidental, EE. UU.), baja frecuencia en Asia y Sudamérica. En nuestro medio ocupa el 2do lugar entre los CA aparato digestivo.
Asociado a la poca ingesta de fibra, Genéticos (poliposis familiar), Colitis Ulcerosa, Pólipo Velloso, Sd de Gardner poliposis y quistes cebáceos, fibromas, osteomas y dentificación anormal. Sme de Cronckite Canada poliposis, aracnodactilia y alopecia. Sme Peutz Jeghers poliposis (hamartomas) con manchas negras en piel y labios. Sme Turcot poliposis y tumor del SNC. Sme de CA familiar o Lynch I – II, CA sincrónicos – se desarrollan al mismo tiempo en el mismo segmento. CA metacrónico – después de un primer CA operado aparece en otro segmento.
Endoscópico – Cuando no operable
Cirugía – siempre intentar en colon cuando no haya metástasis – tumelizacion del TU.
14 comentários:
Peculiar article, exactly what I was looking for.
Also visit my website :: iraqi dinar rv
Do you mind if I quote a few of your articles as long as I provide credit and
sources back to your blog? My website is in the
very same area of interest as yours and my
visitors would definitely benefit from some of
the information you present here. Please let me know if this
alright with you. Thank you!
my site > Lexington Law
each time i used to read smaller articles or reviews which as well clear
their motive, and that is also happening with this article which
I am reading at this place.
my web page > The Tao of Badass Review
magnificent put up, very informative. I ponder why the other experts of this sector don't notice this. You should continue your writing. I'm confident, you have a huge readers' base already!
Feel free to surf my web blog ; click through the next web page
Good article. I will be facing many of these issues as well.
.
Here is my page :: buy zeolite
Good post. I learn something totally new and challenging on
blogs I stumbleupon on a daily basis. It will always be interesting to
read content from other writers and practice a little something from their web sites.
My web page - leadership speakers Gauteng
Hmm is anyone else encountering problems with the images on this blog loading?
I'm trying to determine if its a problem on my end or if it's the blog.
Any feed-back would be greatly appreciated.
My webpage: browse around this web-site
I used to be able to find good info from your blog articles.
My page - visit this website
Oh my goodness! Awesome article dude! Many thanks, However I am experiencing issues with your RSS.
I don't know the reason why I cannot join it. Is there anyone else getting the same RSS problems? Anybody who knows the answer will you kindly respond? Thanks!!
Have a look at my website; http://www.cleanserv.co.za
Amazing! This blog looks just like my old one! It's on a totally different topic but it has pretty much the same page layout and design. Superb choice of colors!
Also visit my web site ... Arabic Books
Hey there, You've done an excellent job. I'll certainly digg it and personally suggest to my friends.
I am confident they will be benefited from this web site.
Also visit my blog post; tao of badass reviews
It is appropriate time to make some plans for the future and
it is time to be happy. I have read this post and
if I could I wish to suggest you few interesting things or advice.
Maybe you could write next articles referring to this
article. I wish to read even more things about it!
Here is my blog post ... solar outdoor lights
Hmm it seems like your site ate my first comment (it was super long) so I guess I'll just sum it up what I wrote and say, I'm thoroughly enjoying your blog.
I too am an aspiring blog writer but I'm still new to everything.
Do you have any tips and hints for rookie blog writers?
I'd really appreciate it.
Also visit my weblog; psychic readings
I am sure this paragraph has touched all the internet people,
its really really fastidious article on building up new website.
Feel free to surf to my web page - zulutrade1.com
Postar um comentário